

Evidence suggests that it isn’t smoking that is the primary driving force behind the worldwide lung cancer epidemic, but sugar. read more

Look at the ingredient label of almost any packaged food you consume and odds are you will spot the term “natural flavors.” Have you ever wondered what this mysterious additive actually contains? read more
Scientists have discovered new evidence that strengthens the link between oral infections and Alzheimer’s disease. read more

Many websites are promoting a caprylic acid-based supplement, referred to as brain fuel, as superior to coconut oil for promoting brain health. Is it really superior or just marketing hype? read more
Smoking has long been believed to be the primary cause of lung cancer. Men who smoke are 23 times more likely to develop lung cancer and women are 13 times more likely, compared to those who have never smoked. Secondhand smoke is nearly as bad; nonsmokers who are exposed to secondhand smoke at home or work have a 20 to 30 percent greater risk of developing this type of cancer.
Lung cancer is the most common cancer worldwide, accounting for 2.1 million new cases and 1.8 million deaths per year (2018). It is by far the leading cause of cancer death among both men and women. Each year, more people die from lung cancer than from colon, breast, and prostate cancer combined.[1]
Smoking is a major risk factor of six of the eight leading causes of death worldwide: heart attack, stroke, lower respiratory infection, chronic obstructive pulmonary disease (COPD), tuberculosis, and lung/bronchial cancer.
Despite the fact that the number of people who smoke has decreased in most countries, the rate of lung cancer remains high. In the United States, for example, the use of tobacco products has been declining since the 1970s, tobacco use is lower now than it has been in a century, yet lung cancer rates have continued to increase, peaking in the 1990s. Since then it has only slightly declined. If smoking causes cancer, why do cancer rates remain high despite the reduction in tobacco use?
While there is no question that smoking contributes to lung cancer and many other health problems, it may not be the primary factor involved. Diet appears to play a significant role. The similarity between lung cancer deaths and sugar consumption is obvious. See the graphs.
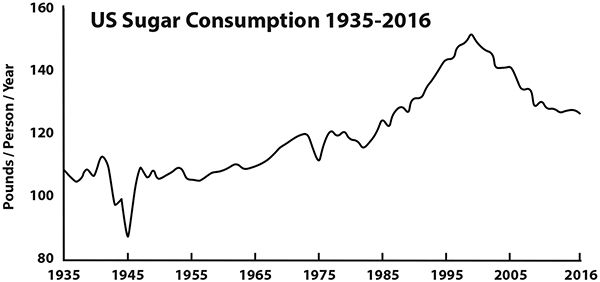
Sugar consumption has risen steadily (with a brief dip during WWII due to rationing) and peaked in 1999 and then has gradually declined.
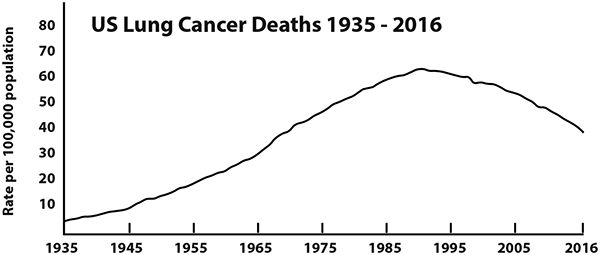
Lung cancer has the same general rise, peaking in the 1990s.
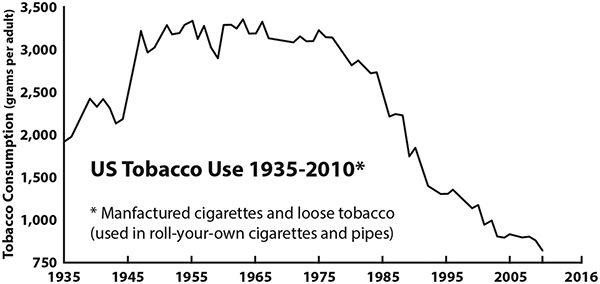
In contrast, the correlation between tobacco use and lung cancer is not as obvious.
It is quite possible that smoking, by itself, may not be enough to cause cancer. Sugar may be the catalyst that makes tobacco so dangerous. In fact, cancer depends on sugar as its primary source of energy. Without sugar, cancer could not survive. [2]
Prior to the mid 1900s, lung cancer was relatively uncommon in the US. In 1930 the death rate due to lung cancer for both men and women was less than 3.5 per 100,000. In 2016 the rate for men was 46.7 and women 31.9 per 100,000; the cancer death rates were much higher even though far fewer people smoked. [3] The number of smokers has decreased while lung cancer deaths have increase over tenfold. There has to be something else going on here.
Smoking has never been a major problem in any population until sugar and refined flour have been added to the diet. A number of primitive societies have used tobacco for generations without suffering any apparent harm. For example, the Inuit of northern Canada and Alaska have traditionally been very heavy smokers. Despite the fact that they lived a nomadic hunter-gatherer lifestyle, they obtained tobacco through trade with other indigenous peoples, who in turn, got it from French, Canadian, and American traders. Tobacco was a primary commodity in trade. Nearly all Inuit smoked. Every evening they would go into their shelters, which were tightly sealed off from the bitter arctic cold, and smoke. The room would fill with tobacco smoke as well as smoke from the fires that keep them warm and give them light, with only one small air vent in the middle of the roof. Everyone, including young children, were exposed to heavy doses of secondhand smoke their entire lives.
The smoking habits of the Inuit were recorded by many of the arctic explorers. In the early 1900s, anthropologist Vilhjalmur Stefansson, who lived with the Inuit for 11 years, described their habitual use of tobacco. If smoking caused lung cancer, the Inuit would definitely have had a cancer epidemic. However, one of the things Stefansson noted was the complete absence of cancer of any type.[4] In addition, none of the major diseases strongly linked to smoking were evident among the Inuit. A diet of antioxidant-rich fruits and vegetables was not what was protecting them. At that time, the Inuit diet consisted almost entirely of meat and fat. They ate no vegetables, fruits, or grains and absolutely no sugar or sweets of any kind, except what little they might get on rare occasions from isolated trading posts.
Before 1955, most Inuit lived a nomadic life, living off the land. Starting in the mid-1950s, the Inuit were recruited to work on military and civilian airports across the Alaskan and Canadian Arctic. By the late 1960s, almost all of the Inuit had given up their nomadic lifestyle and were living in permanent communities. They also gave up their traditional diet and began eating many of the same products as most North Americans—processed flour, sugar, sweets, vegetable oils, and canned goods. Before this time, the Inuit rarely even saw sugar and ate caribou fat and seal blubber by the pound.
Dr. Otto Schaefer, director of the Northern Medical Research Unit of the Charles Camsell Hospital in Edmonton, Canada, worked among the Inuit for more than 20 years and witnessed firsthand the transition that occurred in the 1950s and 1960s. He noted that the traditional high-fat diet was replaced with one high in sugar. In one Inuit community in the Canadian Western Arctic, he was able to get detailed records of food imports spanning eight years, from 1959 to 1967. He found that sugar consumption by the average Inuit in the area quadrupled during that time, from 26 pounds per person per year to 104.2 pounds. [5]
Before living in permanent settlements, degenerative diseases, like diabetes and heart disease, were extremely rare. However, within one decade, the Inuit began experiencing degenerative disease at an alarming rate. Diabetes tripled. Dr. Schaefer noted that in this Inuit community there were more new cases of diabetes than had occurred in all of the Inuit living in the entire country of Canada just a few years earlier. Diseases of the arteries among men over 40 increased fivefold. Gallbladder disease skyrocketed. At one time, all of the Inuit were slim and trim even in middle age, but living in the settlements, they developed bulging paunches.
Cancer, of any type, was never seen in the Inuit who lived on the traditional high-fat diet. Lung cancer was completely absent among them even though they smoked heavily. Dr. Schaefer observed that smoking itself did not cause cancer in the Inuit unless the diet also included sugar. “If smoking alone causes lung cancer,” wrote Dr Schaefer, “we should expect to find many cases of Eskimos and Indians, who almost all smoke quite heavily, mostly cigarettes in recent decades. No bronchogenic cancer had been found [among the natives of Northern Canada.]” [6]
Tens of thousands of Inuit and native Americans throughout North America smoked heavily and were exposed to secondhand smoke from infancy, yet none (zero) of them developed lung cancer until after they began adding sugar and refined carbohydrates into their diets. The absence of lung cancer is not unique to the Inuit and Native Americans, but has been observed in many primitive cultures throughout the world that had a sugar-free diet.

We have all known or heard of people who smoked, and yet lived long healthy lives, free of cancer. A good example is the cigar smoking actor and comedian George Burns. He began smoking at the age of 14 and is reported to have smoked between 10 and 15 cigars a day for over 70 years (more than 300,000 cigars in his lifetime).
Burns remained in good health all his life and was still actively working as a stand-up comedian until just weeks before his death in 1996, at the ripe old age of 100. He exercised regularly, was not overweight, did not have any blood sugar problems, and ate a relatively low-sugar diet. He even wrote a bestselling diet book titled How to Live to Be 100—Or More. Despite his heavy smoking habit, his diet and lifestyle had the greater influence on his health.
Smoking is not benign by any means, it is a risk factor for a multitude of diseases, generates a great deal of oxidative stress, and depletes nutrients essential for good health. However, it appears that smoking itself is not enough to cause lung cancer until it is combined with a high-sugar diet. It is the tobacco-sugar one-two punch that is the real culprit in causing lung cancer.
If you smoke or are around smokers and want to avoid lung cancer or other diseases associated with smoking, your best defense, besides avoiding tobacco, may be a healthy, low-sugar diet.
The link between sugar and cancer, as well as many other chronic diseases is described in my new book Fat Heals, Sugar Kills.
References
1. https://www.cancer.org/cancer/non-small-cell-lung-cancer/about/key-statistics.html
2. http://www.chiro.org/nutrition/FULL/Cancers_Sweet_Tooth.shtml
4. Stefansson, V. Cancer: Disease of Civilization? Hill and Wang: New York, 1960.
5. Schaefer, O. When the Eskimo Comes to Town. Nutrition Today.1971;6:8-16.
6. Schaefer, O. Medical observations and problems in the Canadian arctic. Canad M A J 1959;81:386-393.
Book featured in this article:
Fat Heals, Sugar Kills
The Cause of and Cure for Cardiovascular Disease, Diabetes, Obesity, and Other Metabolic Disorders
by Dr. Bruce Fife
Available from Piccadilly Books, Ltd.
For a description or to order click here
Top of Page
Look at the ingredient label of almost any packaged food you consume and odds are you will spot the term “natural flavors.” Have you ever wondered what this mysterious additive actually contains?
Natural flavors are added to a wide variety of foods ranging from flavored waters and granola bars to frozen dinners and ice cream. You will find it listed on the ingredient label of both organic and conventional foods. According to the Environmental Working Group’s Food Scores database of over 80,000 foods, natural flavor is the fourth most common ingredient listed on labels, appearing on one of every seven labels. The only ingredients that outrank it are salt, water, and sugar.
When you see the natural flavors listed on an ingredient label, you have no clue what chemicals may have been added to the food under this ambiguous term. Natural flavors sounds a whole lot healthier than the presumably chemical-laden alternative—artificial flavors, and is more enticing to customers. But just what are natural flavors anyway? Are they really natural? And what distinguishes them from artificial flavors, or is there any difference? It turns out they may not be all that better.
The US Food and Drug Administration (FDA) has defined natural flavors as those derived from spices, fruits or fruit juice, vegetables or vegetable juice, edible yeast, herbs, bark, buds, roots, leaves or similar plant material, meat, fish, poultry, eggs, dairy products, or fermentation products, essentially anything from plant or animal sources.[1] In contrast, artificial flavors, are man-made chemicals.
For nonorganic foods, the regulations do not restrict ingredients from sources that are irradiated or genetically engineered, or are known to cause problems. For example, MSG, which is often included under the umbrella of natural flavorings, can be considered a natural flavor as it is derived from seaweed, but many people are highly allergic to it and it is a well-documented neurotoxin.

Food companies must list all of the ingredients on a food label; however, flavor manufacturers do not have to disclose their ingredients. They can add synthetic solvents, preservatives, emulsifiers, carriers, and other additives to a flavor that qualifies as natural under current regulations. So, natural flavors may contain unnatural products like preservatives and solvents used in their production. Because of the wide variety of ingredients that typically go into natural flavorings, “there does not seem to be much of a difference between natural and artificial flavors,” said David Andrews, a scientist at the Environmental Working Group, a research and advocacy organization.
“The differentiation is really down to the origin of those molecules, whether synthetically processed in a lab or purified in a lab but from a natural source,” Andrews says. Here's where it gets even muddier: Added flavoring, both natural and artificial, could contain anywhere from 50 to 100 ingredients. And all of the extra ingredients in flavors often aren't as innocent as you'd hope they would be. “The mixture will often have some solvent and preservatives — and that makes up 80 to 90 percent of the volume [of the flavoring]. In the end product, it’s a small amount, but it still has artificial ingredients,” Andrews says. [2]
The case is different with certified organic foods. Natural flavors allowed for use in these foods are subject to a different and far more restrictive set of regulations. There is an extensive list of synthetic solvents, emulsifiers, artificial preservatives, and other substances that cannot be included. They must use non-petroleum-based solvents, cannot be irradiated and cannot use flavor extracts derived from genetically engineered crops.
Flavors labeled “organic flavors” or “organic natural flavors” are even more strictly regulated, consisting almost entirely of organic ingredients; the latter may contain a small amount of natural flavor however.
References
1. https://www.accessdata.fda.gov/scripts/cdrh/cfdocs/cfcfr/cfrsearch.cfm?fr=501.22
Over the past few decades the incidence of Alzheimer’s disease has skyrocketed, from a relatively rare condition to one of the most common causes of death. Dementia is the fifth leading cause of death worldwide. Alzheimer’s is the most common form of dementia, constituting some 70 percent of cases. Yet, researchers have been unable to agree as to what causes it.
Alzheimer’s is characterized by the excessive accumulation of amyloid plaque in the brain. For this reason, it was believed that this sticky plaque interfered with normal brain function leading to Alzheimer’s. Consequently, since 1985 the majority of the research into understanding and treating Alzheimer’s has focused on the “amyloid hypothesis.”
Over the years, huge sums of money have been spent to find ways to prevent or remove this plaque. In 2018 alone, the US National Institutes of Health invested $1.9 billion on Alzheimer’s research. Despite the years of research and money spent, we are no closer the solving the Alzheimer’s mystery than we were 30 years ago. The failure rate of drug development has been essentially 100 percent.[1]
Drugs designed to dissolve the amyloid have proven successful in reducing the plaque, but have failed miserably in stopping progressive memory loss.
In recent years, researchers are realizing that the excessive focus on eliminating amyloid may have been a mistake. Instead of being the cause of Alzheimer’s, it appears to be a result of the body’s means of self preservation. Amyloid forms as a defense against intrusive microorganisms. When researchers injected bacteria into the brains of mice, amyloid plaque developed around the bacteria overnight, preventing the bacteria from spreading.
Bacteria and viruses have been found in the brains of Alzheimer’s patients for many years. But it has not been determined whether the microbes caused the disease or were simply able to enter the brain damaged by Alzheimer’s. It now appears that the formation of plaque is the result of the brain’s effort to protect itself from infection.
It has been known that Alzheimer’s patients have a higher incidence of gum disease than the general population. The primary bacterium that causes gum disease is Porphyromonas gingivalis. This bacterium is also known to invade and infect the regions of the brain affected by Alzheimer’s. In animal studies, P. gingivalis introduced into the brain leads to the formation of amyloid plaque and symptoms consistent with Alzheimer’s.
Researchers from Cortexyme, a pharmaceutical firm in San Francisco, have found evidence of P. gingivalis in up to 99 percent of Alzheimer’s patients studied.[2] Researchers at the University of Central Lancashire, UK, have found that P. gingivalis actively invades the brains of mice with gun infections.[3] Based on this research, it is now becoming clear that brain infections can be a major factor in Alzheimer’s.
The mouth is home to a diverse community of microorganisms. When dental plaque builds under the gums, it can form inflamed pockets that damage the lining of the mouth, which can make it possible for P. gingivalis and other bacteria and viruses to seep into the bloodstream spreading to the brain and other parts of the body. Even if you don’t have gum disease, transient damage to your mouth lining from eating, tooth-brushing, or routine dental care, can allow mouth bacteria into your bloodstream.
The blood-brain barrier normally keeps out most microbes, however, some bacteria and viruses are known to gain entry by invading cranial nerves near the mouth and nose and spread into the brain.
P. gingivalis isn’t the only microbe that has been found in the amyloid plaque of Alzheimer’s brains. Other microorganisms include spirochetes, herpes virus, Chlamydia pneumonia, Epstein-Barr virus, Helicobacter pylori, and cytomegalovirus, all of which are known to inhabit the mouth.[4-8]
Spirochetes are well documented causes of neurodegenerative disease. [9-10] In postmortem examinations of brain tissues, researchers from Oregon Health and Sciences University School of Dentistry looked for evidence of two species of oral spirochetes known to cause periodontal disease. They detected evidence of these spirochetes in brain tissue in 14 of 16 samples from subjects with Alzheimer’s disease, but only 4 or 18 in samples from control subjects.[11] In the mouth, these bacteria cause inflammation, ulcers, pus, and tissue decay. They can do the same in the brain.
In another study, researchers found spirochetes in all 14 autopsy cases of Alzheimer’s examined, but failed to find them in any of the 13 age-matched subjects who did not have the disease,[12] providing further evidence to the strong involvement bacteria may play in Alzheimer’s disease. Spirochetes are believed to invade the brain through the cranial nerves.[13]
Most of us have the bacterium Chlamydia pneumonia, living in our sinuses and mouths. While it is a common cause of pneumonia, and is often associated with sinusitis, laryngitis, bronchitis, asthma, and other respiratory problems it can also cause periodontal disease. Like P. gingivalis and spirochetes, Chlamydia, can find entry into the brain through the cranial nerves and has been found in the amyloid plaque of those with Alzheimer’s.
In one study, investigators analyzing brain tissue from deceased Alzheimer’s patients found the bacterium in the brains of 17 out of 19 Alzheimer’s patients, while in age-matched non-Alzheimer’s brain tissue it was found in only 1 out of 19 cases.[14] In another study, investigators found the bacterium in 90 percent of the subjects studied. In comparison, only 5 percent of non-Alzheimer’s brains contained this bacterium.[15]
In addition, when mice were exposed to a nasal spray containing the bacterium, they developed the same senile plaques in their brains, providing further proof that this bacterium triggers amyloid plaque formation.[16]
Viruses, too, can find their way into the brain. Herpes simplex type 1 (oral herpes) infects the vast majority of the population and up to 90 percent of the elderly.[17] Herpes can be involved in periodontal disease, but is most commonly associated with cold sores on the lips. Once a person is infected, the virus remains for life, generally hiding dormant in the cranial nerves in the mouth and sinus cavity. Flare-ups occur from time to time causing the distinctive lesions on the lips. Since the virus hides inside the cranial nerves, it is easy for it to migrate into the brain.
When the virus is added to cultured brain cells, it results in a dramatic increase in amyloid. Likewise, in rat brains the virus causes the proliferation of amyloid.[18] In human studies, evidence of herpes virus has been found in 90 percent of the plaque examined in Alzheimer’s brains.[19]
It is interesting that several oral microorganisms have been found to be associated with Alzheimer’s disease. Judith Miklossy, MD, PhD, of the University of British Columbia, and author of numerous studies on infectious causes of Alzheimer’s, states that “co-infection of spirochetes with other bacteria, including Chlamydia and herpes, is frequent.”[20] That makes sense. A person with a history of dental problems would have an overgrowth of many types of microorganisms in their mouths and consequently, several of these would likely escape from the mouth and find their way in the brain. The amyloid plaque in Alzheimer’s brains is probably the result of the invasion of several types of oral microorganisms rather than just one.
Antibiotics have not proven to be successful in treating Alzheimer’s. Most of these drugs cannot pass across the blood-brain barrier. Cortexyme, the pharmaceutical company investigating the link between P. gingivalis and Alzheimer’s, is developing a drug to block the toxins produced by the bacterium in hopes that it may have a positive effect.
However, the problem with treating Alzheimer’s against a single microbe, like P. gingivalis, is that it is only one of many organisms that can enter and infect the brain. If you block P. gingivalis, that won’t stop spirochetes or Chlamydia. Drugs designed to kill or inhibit bacteria are useless against viruses, so herpes and other viruses would be unfazed.
An alternative approach would be to use coconut oil as described in my book Stop Alzheimer’s Now. The medium chain fatty acids in coconut oil have been shown to kill most of the bacteria and viruses that have been found associated with Alzheimer’s. Lauric acid, the primary medium chain fatty acid in coconut oil also stimulates the production of white blood cells, boosting immune function. Consuming coconut oil on a regular basis can reduce the risk of infection from these microbes.
Since most of the microorganisms found associated with Alzheimer’s appear to originate from gum infections it makes sense to also focus on oral health. In addition to regular dental care, oil pulling would be immensely helpful. Oil pulling is the process of swishing a spoonful of oil (preferable coconut oil) in the mouth for several minutes and then spitting it out. The process of swishing the oil “pulls” bacteria and viruses out from around the teeth and gums and out of infected pockets, thus greatly reducing the microbial load in the mouth and clearing out infected pockets. Studies have shown that oil pulling reduces the amount of potentially harmful germs better than the strongest antimicrobial mouthwashes and effectively reduces gum disease and plaque.
References
1. Cummings, J., et al. The price of progress: Funding and financing Alzheimer’s disease drug development. Alzheimer’s & Dementia: Translational Research & Clinical Interventions 2018;4:330-343.
2. Dominy, SS, et al. Porphyromonas gingivalis in Alzheimer’s disease brains: Evidence for disease causation and treatment with small molecule inhibitors. Science Advances 2019;5;eaau3333.
3. Sophie, P, et al. Activation of Porphyromonas gingivalis and infection-induced complement activation in ApoE-/- mice brains. Journal of Alzheimer’s Disease 2015;43:67-80.
4. Volpi, A. Epstein-Barr virus and human herpesvirus type 8 infections of the central nervous system. Herpes 2004;11 Supple 2:120A-127A.
5. Honjo, K., et al. Alzheimer’s disease and infection: do infectious agents contribute to progression of Alzheimer’s disease? Alzheimers Dement 2009;5:348-360.
6. Meer-Scheerer, L., et al. Lyme disease associated with Alzheimer’s disease. Curr Microbiol 2006;52:330-332.
7. Itzhaki, R.F., et al. Infiltration of the brain by pathogens causes Alzheimer’s disease. Neurobiol Aging 2004;25:619-627.
8. Kountouras, J., et al. Association between Helicobacter pylori infection and mild cognitive impairment. Eur J Neurol 2007;14:976-982.
9. Miklossy, J. Chronic inflammation and amyloidogeneis in Alzheimer’s disease—role of spirochetes. Journal of Alzheimer’s Disease 2008;13:381-391.
10. Miklossy, J., et al. Beta-amyloid deposition and Alzheimer’s type changes induced by Borrelia spirochetes. Neurobiol Aging 2006;27:228-236.
11. Riviere, G.R., et al. Molecular and immunological evidence of oral Treponema in the human brain and their association with Alzheimer’s disease. Oral Microbiol Immunol 2002;17:113-118.
12. Miklossy, J. Alzheimer’s disease—a spirochetosis? Neuroreport 1993;4:841-848.
13. Balin, B.J., et al. Chlamydophila pneumoniae and the etiology of late-onset Alzheimer’s disease. Journal of Alzheimer’s Disease 2008;13:371-380.
14. Balin, B.J., et al. Identification and localization of Chlamydia pneumonia in the Alzheimer’s brain. Med Microbiol Immunol 1998;187:23-42.
15. Gerard, H.C., et al. Chlamydophila (Chlamydia) pneumonia in the Alzheimer’s brain. FEMS Immunol Med Microbiol 2006;48:355-366.
16. Little, C.S., et al. Chlamydia pneumoniae induces Alzheimer-like amyloid plaques in brains of BALA/c mice. Neurobiol Aging 2004;25:419-429.
17. Itzhaki, R.F. and Wozniak, M.A. Herpes simplex virus type 1 in Alzheimer’s disease: The enemy within. Journal of Alzheimer’s Disease 2008;13:393-405.
18. Wozniak, M.A., et al. Herpes simplex virus infection causes cellular beta-amyloid accumulation and secretase upregulation. Neurosci Lett 2007;429:95-100.
19. Wozniak, M.A., et al. Herpes simplex virus type 1 DNA is located within Alzheimer’s disease amyloid plaques. J Pathol 2009;217:131-138.
20. Miklossy, J. Chronic inflammation and amyloidogeneis in Alzheimer’s disease—role of spirochetes. Journal of Alzheimer’s Disease 2008;13:381-391.
Books featured in this article:
Stop Alzheimer's Now!
How to Prevent and Reverse Dementia, Parkinson's, ALS, Multiple Sclerosis, and Other Neurodegenerative Disorders
by Dr. Bruce Fife
Available from Piccadilly Books, Ltd.
For a description or to order click here
Oil Pulling Therapy
Detoxifying and Healing the Body Through Oral Cleansing
by Dr. Bruce Fife
Available from Piccadilly Books, Ltd.
For a description or to order click here
Top of Page
With the publication of my book Stop Alzheimer’s Now and the publication of a number of studies demonstrating the effectiveness of treating brain disorders with coconut oil and medium chain triglycerides (MCTs), coconut oil has gained a reputation as a brain boosting food.[1-5]
The reason why coconut oil is able to support healthy brain function is due to the MCTs in the oil. MCTs are composed of medium chain fatty acids (MCFAs). Three MCFAs, plus a glycerol molecule, makes one MCT molecule. Coconut oil is composed of about 63 percent MCFAs in the form of MCTs. When consumed, MCTs are broken down into individual medium chain fatty acids. Most these MCFAs go directly to the liver where they are converted into ketones. Ketones are a high-potency fuel that can cross over the blood-brain barrier and nourish the brain.
Chronic inflammation, which is common in most all types of brain disorders including Alzheimer’s, Parkinson’s, ALS, Huntington’s, autism, stroke, traumatic brain injury, and others, causes insulin resistance. Consequently, brain cells are unable to effectively absorb glucose, its main source of energy, causing neurons to degenerate and die, leading to the symptoms associated with these disorders.
Ketones, however, are not affected by this defect in glucose metabolism. Brain cells can easily absorb ketones even in a state of insulin resistance. Ketones also activate special proteins in the brain called brain derived neurotrophic factors that regulate brain cell function, maintenance, repair, and growth and protect the brain from oxidative stress and runaway inflammation. Neurotrophic factors also stimulate the growth of new brain cells to replace old or damaged cells. Consequently, ketones can have a very pronounced effect on brain health and can be used therapeutically to treat many brain disorders. Since the MCTs in coconut oil are converted into ketones, coconut oil has gained a reputation as a natural brain food.
MCT oil, which consists of 100 percent MCTs, has also been effective in treating brain disorders and boosting brain function. Many people assume that MCT oil is superior to coconut oil for treating brain disorders because of its higher MCT content.
MCT oil, which consists of 100 percent MCTs, has also been effective in treating brain disorders and boosting brain function. Many people assume that MCT oil is superior to coconut oil for treating brain disorders because of its higher MCT content.


Coconut oil is composed primarily of lauric acid, a 12 carbon chain (C12) MCFA, accounting for about 48 percent of the oil. It also contains 8 percent caprylic acid, an 8 carbon chain (C8) MCFA; 7 percent capric acid, a 10 carbon chain (C10) MCFA; and about 0.5 percent caproic acid, a 6 carbon chain (C6) MCFA; with the remaining 36.5 percent consisting of various longer chain fatty acids.
MCT oil, on the other hand, is composed entirely of just two fatty acids—caprylic and capric acid. It contains no lauric acid.
The smaller the carbon chain, the quicker and more efficiently MCFAs are converted into ketones by the liver. Therefore, caprylic acid (C8) is rapidly converted into ketones, with capric acid (C10) a little slower, and lauric acid (C12) slower still. When consumed, MCT oil raises blood ketone levels quicker and higher than coconut oil. For this reason, many people have assumed that MCT oil is superior to coconut oil in treating brain disorders.
Some enterprising individuals have taken this concept a step further and have produced products containing pure caprylic acid (C8), claiming it boosts ketones higher and faster than either coconut oil or MCT oil and, therefore, is a superior source for raising blood ketone levels and boosting brain function. They give their products names such as MCT Oil Brain Fuel or Brain Octane Oil.
These products are sold at a premium price. The most popular brand is Bulletproof Brain Octane Oil; a 16 ounce bottle retails for $30. A serving size is 1 tablespoon and each bottle contains 32 servings for a price of $0.94 or nearly $1 per serving. In contrast, 1 tablespoon serving of coconut oil sells for about $0.20. Does the benefit justify the price difference?
Because of the huge difference in price, sellers try to inflate the benefits of pure caprylic acid and emphasis the perceived shortcomings of coconut oil, even to the point of distorting the truth. Sellers of this Brain Octane claim that lauric acid isn’t even a MCFA at all and is really a long chain triglyceride (LCT) in order to deceive customers. I ask: if Brain Octane is so superior to coconut oil why do the sellers have to resort to lies to sell their product?
Is Brain Octane really superior to coconut oil? The claim is that it raises blood ketones higher and faster than coconut oil. Pure caprylic acid does, indeed, do this, but blood levels peak in about 1.5 hours after taking it and is completely gone in about 3 hours. While coconut oil does not raise blood ketones as high, it does raise it enough to have therapeutic value and peaks after about 3 hours and remains elevated for a full 8 hours. You would have to take over 5 tablespoons of Brain Octane to equal the duration of an equal amount of coconut oil. This is impractical since taking more than 1 tablespoon of pure caprylic acid can cause severe stomach cramping and diarrhea. Coconut oil is by far gentler on the stomach and you can take 2 or more tablespoons at a time to boost ketone levels higher. Duration is a big issue when it comes to degenerative brain diseases like Alzheimer’s because if the brain does not have a steady source of ketones available 24 hours a day to supply its energy needs, it begins to die. Maintaining a steady source of ketones prevents this. For this reason, coconut oil provides the greater overall benefit.
In order to keep blood ketones elevated for 24 hours a day it would require taking caprylic acid at least 8 times a day or once every 3 hours day and night. Taking so much caprylic acid would cause harsh digestive stress, abdominal cramping, and severe diarrhea. Since it would also be needed at night, you would have to wake up repeatedly to take the supplement, preventing a good night’s sleep. Consequently, the sellers of the product only recommend that it be taken once or twice a day.
In contrast, coconut oil only needs to be taken two to three times a day and need not be taken during the night to maintain ketone levels. It is also much gentler on the digestive system.
The biggest selling point made by those pushing these products is the claim that caprylic acid is better than coconut oil because it raises blood ketone levels higher than lauric acid. It is true that “blood” ketones rise higher with caprylic acid, however, that is not the same as “brain” ketones, which is the real issue. The fact of the matter is, lauric acid can raise brain ketones as high or higher than caprylic acid and it is in the brain where you want the ketones, if your goal is to boost brain health.
Researchers at the University of Tokyo discovered that lauric acid, if not converted into ketones immediately by the liver, will travel directly to the brain and be converted to ketones by the brain itself.[6] The researchers stated that “These results suggest that coconut oil intake may improve brain health directly activating ketogenesis in astrocytes and thereby by providing fuel to neighboring neurons.”
Coconut oil has been shown to be very useful in the treatment of Alzheimer’s disease. One of the characteristics of Alzheimer’s disease is the formation of sticky amyloid plaque in the brain. (See the previous article “Has the Elusive Cause of Alzheimer’s been Found?) In a study by Canadian researchers both coconut oil and lauric acid were shown to reduce the formation of amyloid plaque, thus promoting neuron survival.[7] It must be pointed out that it is the lauric acid in coconut oil that has this effect. Caprylic acid will have little if any affect on the amyloid plaque. The reason for this is that caprylic acid is either absorbed in the intestines and used immediately as fuel or converted into ketones by the liver. Ketones have no antimicrobial effect and cannot defend the brain against infection. Although caprylic acid does have some antimicrobial effect, none of it can reach the brain to defend against infection. Lauric acid, on the other hand, is partly converted into ketones by the liver, while the rest enters the bloodstream where it can reach the brain and defend it against infection as well as be converted into ketones.
Autopsies on the brains of deceased Alzheimer’s patients have found a high percentage of them to be infected by the herpes virus. The virus is believed to be directly involved in the formation of amyloid plaque in brain tissue. Evidence of herpes virus have been found in 90 percent of the plaque examined in Alzheimer’s brains, strongly implicating a connection between the virus and Alzheimer’s disease.[8] Lauric acid has the greatest anti-herpes potential of all the MCFAs. For this reason, many Alzheimer’s patients do better with coconut oil than they do with MCT oil alone. Many people have successfully used coconut oil to treat family members with Alzheimer’s. However, when they switched to using only MCT oil, because they were told it raised ketone levels higher, they saw a distinct decline in mental health and went back to using coconut oil or a combination of coconut and MCT oils.
Coconut oil has proven to be highly successful in raising blood ketones to therapeutic levels and in the treatment of brain related disorders including, Alzheimer’s, Parkinson’s, autism, glaucoma, and others.[9-11] In animal studies, it has proven to have potential as a memory enhancer. The researchers attributed much of this effect to coconut oil’s antioxidant effect derived from all of its MCFAs.[12]
It is apparent that coconut oil has very pronounced therapeutic effects on brain health. Despite the negative comments about coconut oil and lauric acid by marketers selling the various brands of brain fuel, you are likely to get better results by combining coconut oil with these products or by just sticking to pure coconut oil.
References
1. Fernando, WMADB, et al. The role of dietary coconut for the prevention and treatment of Alzheimer’s disease: potential mechanisms of action. Brit J Nutr 2015;114:1-14.
2. Chintapenta, M, et al. A brief review of caprylidene (Axona) and coconut oil as alternative fuels in the fight against Alzheimer’s disease. Consult Pharm 2017;32:748-751.
3. Cunnane, SC, et al. Can ketones help rescue brain fuel supply in later life? Implications for cognative health during aging and the treatment of Alzheimer’s disease. Front Mol Neurosci 2016;Jul 8;9:63.
4. Hu Yang, I, et al. Coconut oil: non-alternative drug treatment against Alzheimer’s disease. Nutr Hosp 2015;32:2822-2827.
5. De la Rubia Orti, JE, et al. How does coconut oil affect cognitive performance in Alzheimer patients? Nutr Hosp 2017;34:352-356.
6. Nonaka, Y, et al. Lauric acid stimulates ketone body production in the KT-5 astrocyte cell line. J Oleo Sci 2016;65:693-699.
7. Nafar, F, et al. Coconut oil protects cortical neurons from amyloid beta toxicity by enhancing signaling of cell survival pathways. Neurochem Int 2017;105:64-79.
8. Wozniak, MA, et al. Herpes simplex virus type 1 DNA in located within Alzheimer’s disease amyloid plaques. J Pathol 2009;217:131-138.
9. Fife, B. Stop Alzheimer’s Now! How to Prevent and Reverse Dementia, Parkinson’s, ALS, Multiple Sclerosis, and Other Neurodegenerative Disorders. Piccadilly Books, Ltd.: Colorado Springs, CO; 2011.
10. Fife, B. Stop Autism Now! A parent’s Guide to Preventing and Reversing Autism Spectrum Disorders. Piccadilly Books, Ltd.: Colorado Springs, CO; 2012.
11. Fife, B. Stop Vision Loss Now! Prevent and Heal Cataracts, Glaucoma, Macular Degeneration, and Other Common Eye Disorders. Piccadilly Books, Ltd.: Colorado Springs, CO; 2015.
12. Rahim, NS, et al. Enhanced memory in Wistar rats by virgin coconut oil is associated with increased antioxidative, cholinergic activities and reduced oxidative stress. Pharm Biol 2017;55:825-832.